South African Type‑2 Diabetes Patients Get Metformin While Insulin Access Lags Behind
For millions of South Africans with type-2 diabetes, the first treatment offered is metformin — a cheap, well-tolerated pill that has been the backbone of diabetes care for decades. Insulin, by contrast, is often reserved for when blood sugar remains dangerously high or complications have already set in. This metformin-first approach, enshrined in national guidelines, is increasingly contested. The UK Prospective Diabetes Study (UKPDS), published in the 1990s, showed that metformin reduced diabetes-related endpoints in overweight patients and was associated with less weight gain and fewer hypoglycemic episodes than insulin or sulfonylureas. However, a growing body of evidence, including the ORIGIN trial, suggests that earlier use of insulin, particularly in patients with severe insulin resistance, could preserve beta-cell function and reduce long-term complications. But in a resource-constrained public health system, the debate is not just about science — it is about cost, logistics, and equity.
Metformin First, Insulin When It's Too Late
South Africa's public-sector diabetes protocol follows a stepwise approach. Patients diagnosed with type-2 diabetes are started on metformin, often at a dose of 500 mg twice daily, with dose adjustments based on HbA1c levels. Only when HbA1c remains above target despite maximum tolerated metformin — and after adding a second oral agent like a sulfonylurea — is insulin considered. In practice, this means many patients spend years on oral therapy alone, even as their glycemic control deteriorates.
The rationale for this sequence is partly historical. The UKPDS showed that metformin reduced diabetes-related endpoints in overweight patients and was associated with less weight gain and fewer hypoglycemic episodes than insulin or sulfonylureas. Subsequent trials, such as ADVANCE, reinforced the safety of intensive glucose control but did not specifically test early insulin. Guidelines worldwide, including those from the World Health Organization, adopted metformin as first-line therapy. Yet South Africa's population has a high prevalence of insulin resistance, driven by genetic predisposition, rising obesity rates, and early-life nutritional factors. Some endocrinologists argue that metformin alone is insufficient for many patients. Dr. Nomsa Mkhize, a diabetologist at Chris Hani Baragwanath Hospital in Soweto, notes that “we see patients who have been on metformin for five years with HbA1c levels above 10% — they are essentially untreated. By the time we start insulin, they already have retinopathy or nephropathy.”
The delay is not merely a matter of guideline inertia. Initiating insulin requires patient education, monitoring, and access to supplies — steps that are often deferred in busy clinics where staff are stretched. A 2023 audit in KwaZulu-Natal found that the median time from diagnosis to insulin initiation was 7.2 years, by which point many patients had developed microvascular complications. Critics say this is too late to prevent the progressive decline of beta-cell function.
Why Insulin Access Stalls Despite Rising Need
Insulin access in South Africa is hampered by a combination of cost, logistics, and training gaps. In the private sector, a month's supply of basal insulin can cost between ZAR 200 and ZAR 400 — roughly 10 to 20 times the cost of metformin. Even with partial insurance coverage, out-of-pocket expenses deter many patients. In the public sector, insulin is provided free of charge, but procurement is limited by budget constraints. The national tender for insulin is renegotiated periodically, but prices remain higher than in many other low- and middle-income countries.
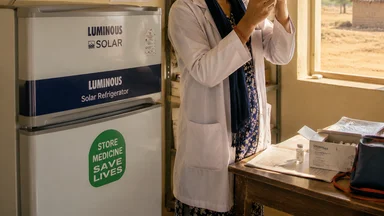
Cold chain logistics pose another barrier. Insulin must be stored at 2–8°C from manufacture to injection. In rural clinics, particularly in the Eastern Cape and Limpopo, power outages and lack of refrigerators can compromise storage. Community health workers sometimes transport insulin in coolers over long distances, but temperature excursions are common. A 2022 study in the South African Medical Journal found that up to 15% of insulin samples collected from rural clinics had degraded due to improper storage.
Shortage of trained nurses for injection education is a further bottleneck. Insulin initiation requires teaching patients how to inject, rotate sites, and recognize hypoglycemia. In many clinics, this task falls to a single nurse who may see dozens of patients per day. “We have to prioritize — those with the highest blood sugar get insulin education, but others are put on a waiting list that can be months long,” says Sr. Thandi Dlamini, a diabetes nurse at a community health centre in Tshwane.
Fear of hypoglycemia among both providers and patients also slows uptake. Hypoglycemia can be severe, especially in patients with irregular meals or limited access to glucose monitoring. Providers worry about causing harm, and patients fear the social stigma of a “low sugar” episode. This risk is not unfounded: a 2021 study in Cape Town reported that 8% of insulin-treated patients had at least one severe hypoglycemic event requiring emergency care over a two-year period.
The Evidence Gap That Drives the Controversy
The debate over early insulin use in type-2 diabetes hinges on whether the benefits of preserving beta-cell function outweigh the risks and costs. The UKPDS did not randomize patients to early insulin, but observational data from its follow-up suggested that patients who received insulin earlier had better long-term glycemic control. More recent trials, such as the ORIGIN trial, found that basal insulin added to oral therapy reduced the risk of cardiovascular events in patients with impaired fasting glucose, though the effect was modest.
However, these trials were conducted largely in high-income settings with homogeneous populations. South African patients often have a different phenotype: young-onset diabetes, high body mass index, and profound insulin resistance. Dr. Bongani Mayosi, a cardiologist at the University of Cape Town, argues that “we cannot simply extrapolate from European trials. Our patients may need a more aggressive approach from the start.” He points to a small study from Durban that showed early insulin therapy (within one year of diagnosis) improved beta-cell function and reduced HbA1c by 2.1% on average compared with metformin alone.
Others counter that the evidence is not strong enough to justify a wholesale shift. Professor Linda-Gail Bekker, an infectious disease specialist who has worked in diabetes care, notes that “metformin is safe, cheap, and effective for many. The real problem is that we don't have enough data from African populations to know who will benefit from early insulin. We need pragmatic trials that compare strategies in our context.” She advocates for a risk-stratified approach, where patients with high HbA1c, young age, or evidence of beta-cell dysfunction are offered insulin earlier.
The controversy is not just academic. In 2024, the South African Diabetes Society updated its guidelines to recommend considering insulin earlier in patients with HbA1c above 9% at diagnosis, but implementation has been uneven. Some provinces have adopted the change; others have not. The lack of consensus reflects a deeper tension between evidence-based medicine and real-world constraints.
To illustrate the practical implications, consider a 45-year-old male patient in Soweto diagnosed with type-2 diabetes and an HbA1c of 10.5%. Under current guidelines, he would start metformin and a sulfonylurea. If his HbA1c remains above 8% after six months, insulin would be considered. However, by that time, his beta-cell function may have declined further. A risk-stratified approach would initiate insulin at diagnosis, potentially preserving his own insulin production. A 2023 modeling study from the University of the Witwatersrand suggested that early insulin in such patients could reduce the incidence of retinopathy by 25% over five years, though the upfront cost would be higher.
A Tale of Two Clinics: Urban vs Rural Reality
In a well-resourced Johannesburg hospital, the diabetes clinic runs twice a week. Patients have access to HbA1c testing on site, a dietitian, and a nurse educator who can initiate insulin in a single visit. Those who need insulin are given a starter pack with syringes, alcohol swabs, and a glucose meter. Follow-up is scheduled within two weeks. The clinic maintains a registry of insulin-treated patients, tracking HbA1c, weight, and hypoglycemia episodes.
Contrast this with a clinic in the rural Eastern Cape, where the nearest hospital is 60 kilometres away. The clinic has a single nurse who sees 80 patients a day. HbA1c testing is done only quarterly by a visiting team. Insulin is dispensed monthly, but supplies sometimes run out. Patients who miss their appointment may go without insulin for weeks. Many rely on traditional healers or simply stop taking medication when they feel well.
Geographic inequity drives divergent treatment paths. Urban patients are more likely to receive insulin earlier and achieve better glycemic control. Rural patients are often diagnosed only after complications — a foot ulcer, blurred vision, or kidney failure — have already developed. A 2023 analysis of the National Health Laboratory Service data found that rural patients had a mean HbA1c of 11.2% at diagnosis, compared with 9.1% in urban areas.
The consequences are stark. Amputation rates for diabetic foot disease are three times higher in rural provinces like the Eastern Cape than in Gauteng. End-stage renal disease from diabetes is also more common, placing additional strain on dialysis services that are already overburdened. These outcomes are not inevitable, but they reflect a system where insulin access is determined more by geography than by clinical need.
Another concrete example: In Limpopo province, a 38-year-old woman with type-2 diabetes and an HbA1c of 11.8% was started on metformin alone at a rural clinic. She developed a foot ulcer within six months, requiring amputation of two toes. Had she received insulin and education earlier, her outcome might have been different. Her story is not unique — similar cases are documented in a 2024 case series from the University of Limpopo.
Cost as the Unspoken Gatekeeper
Even when insulin is clinically indicated, cost remains a formidable barrier. In the public sector, insulin is free at the point of care, but the indirect costs — travel, lost wages, and time away from work — can be prohibitive. A patient living in a rural area may need to spend a full day travelling to collect insulin, missing a day's wage. Some patients ration insulin by skipping doses or using expired supplies, leading to poor glycemic control and increased risk of complications.
In the private sector, out-of-pocket expenses are even higher. A month's supply of basal insulin analogue (like insulin glargine) can cost ZAR 350–400, while human insulin (NPH) is slightly cheaper but still around ZAR 150–200. Metformin, by contrast, costs roughly ZAR 30 per month in the public sector. For a household earning ZAR 3,000 per month, the difference is significant. “I have patients who choose between buying insulin and feeding their children,” says Dr. Mkhize. “It's a choice no one should have to make.”
Health insurance covers insulin for the 16% of South Africans who have private cover, but even then, co-payments and deductibles can add up. The government's proposed National Health Insurance (NHI) scheme aims to improve access, but its implementation has been delayed and its funding uncertain. In the meantime, the cost of insulin remains a de facto gatekeeper, particularly for those with lower incomes.
International comparisons highlight the disparity. In Brazil, insulin is produced locally and costs roughly US$ 5 per vial. In South Africa, the same vial may cost US$ 15–20. Advocacy groups like the T1International movement have called for price reductions and voluntary licensing, but progress has been slow. The South African government has explored compulsory licensing, but legal challenges from pharmaceutical companies have stalled the process.
To put it in perspective, a 2025 analysis by the South African Health Economics Unit estimated that universal insulin access would require an additional ZAR 1.2 billion annually, but could save ZAR 3.5 billion in avoided complications and hospitalizations. The cost-benefit ratio favors investment, yet political will remains elusive.
What Practitioners Are Doing on the Ground
Despite the systemic barriers, some clinicians are finding ways to expand insulin access. In Cape Town, a group of general practitioners has started a “rapid insulin initiation” program for newly diagnosed patients with HbA1c above 10%. They prescribe insulin from the first visit, along with intensive education and weekly follow-up phone calls. Early results, presented at a 2025 conference, showed a 1.8% reduction in HbA1c over six months with no increase in severe hypoglycemia.
Nurse-led education programs have also shown promise. In the Western Cape, a task-shifting initiative trains professional nurses to initiate and titrate insulin independently, under the supervision of a doctor. The program, called “Insulin Start,” has been rolled out to 50 clinics and has reduced waiting times from months to weeks. A 2024 evaluation found that patients in the program had better glycemic control and higher treatment satisfaction than those in usual care.
Community health workers play a crucial role in tracking defaulters. In KwaZulu-Natal, a peer support network called “Sisters for Diabetes” pairs newly diagnosed patients with trained volunteers who have lived experience of diabetes. The volunteers visit homes, remind patients about appointments, and help with injection technique. A small randomized trial suggested that this intervention reduced HbA1c by 0.5% more than standard care.
Clinics are also adapting by using premixed insulin to simplify dosing. Premixed insulin (a combination of rapid- and intermediate-acting insulin) requires only one or two injections per day and is easier to teach than basal-bolus regimens. While not ideal for all patients, it can be a pragmatic solution in settings where resources are limited. “We use premixed insulin as a bridge,” says Sr. Dlamini. “It's not perfect, but it's better than nothing.”
Another innovative approach is the use of telemedicine for insulin titration. In Gauteng, a pilot program used WhatsApp to send daily glucose readings to a nurse who adjusted insulin doses remotely. A 2024 study found that this approach achieved similar glycemic control to in-person visits, with lower costs and fewer missed appointments. Scaling such programs could help rural patients access specialist care without traveling long distances.
Bridging the Gap: Policy Levers That Could Work
Several policy interventions could reduce the insulin access gap. Centralized procurement, similar to the model used for antiretroviral drugs, could lower prices through bulk purchasing and negotiation. South Africa's experience with HIV treatment shows that large-scale procurement can drive down costs — the price of first-line antiretroviral therapy fell by over 80% between 2000 and 2010. A similar approach for insulin could make it more affordable.
Task-shifting insulin initiation to nurses, already piloted in some provinces, should be scaled nationally. This would require regulatory changes, training curricula, and ongoing supervision. The World Health Organization has endorsed task-shifting for diabetes care, and evidence from other countries — such as Ethiopia and Thailand — suggests it is feasible and safe.
Fixed-dose combinations of basal insulin with GLP-1 receptor agonists, such as insulin degludec/liraglutide, are emerging as a convenient option that could reduce the number of injections and improve adherence. However, these products are expensive and not yet available in the public sector. Price negotiations and voluntary licensing could make them more accessible in future.
Diabetes registries could help identify patients who need insulin escalation. The South African National Diabetes Registry, launched in 2022, currently covers only a fraction of public-sector patients. Expanding it and linking it to clinical decision support tools could flag patients with persistently high HbA1c and prompt earlier insulin initiation. Such registries have been shown to improve outcomes in other chronic diseases.
Finally, international donors could subsidize insulin for the public sector. The Global Fund, which primarily focuses on HIV, TB, and malaria, has recently expanded its mandate to include non-communicable diseases. South Africa could apply for funding to support insulin procurement, particularly in rural areas. Similar initiatives have been successful in Rwanda and Malawi.
None of these solutions is a silver bullet. The controversy over when to start insulin will continue as long as evidence remains incomplete and resources are constrained. But the status quo — where patients wait years for insulin while their beta cells decline — is not acceptable. A pragmatic, equity-focused approach that combines better evidence, lower costs, and innovative delivery models can begin to close the gap.
This article is for educational purposes only and does not provide personalized medical advice. Readers should consult their healthcare provider for guidance on diabetes management.