Mumbai Textile Workers Develop COPD While Public Spirometry Tests Cost a Week's Pay
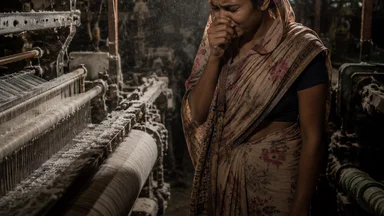
On a humid morning in Bhiwandi, a town northeast of Mumbai that hums with the clatter of thousands of powerlooms, 38-year-old Shabana Sheikh pauses halfway through winding a spool of cotton yarn. She leans against a concrete pillar, coughs into her dupatta, and waits for the tightness in her chest to ease. She has been working in textile units since she was 16. For the past three years, she has noticed that by early afternoon she cannot take a full breath without coughing. Her husband, also a loom operator, tells her it is the same for everyone in the shed. She has never had a spirometry test. When a neighbour went to a private clinic in Bhiwandi and paid ₹600 for one, Shabana decided that was money she could not spare.
A Spirometry Test Costs More Than a Week's Wages for Mumbai's Textile Workers
In the powerloom belt stretching from Bhiwandi to Malegaon, a basic spirometry test at a private clinic typically costs between ₹500 and ₹700. That is roughly the amount a weaver earns in two days—or, for a worker paid on piece rate, the equivalent of a full week's wages after factoring in lost time. The daily wage for a powerloom worker in this region ranges from ₹300 to ₹400, according to a 2024 survey by the Self-Employed Women's Association (SEWA). For a family of four, that income barely covers rent, food, and children's school fees. Spending ₹600 on a test that might reveal bad news is a luxury many cannot afford.
Public hospitals in Mumbai and nearby Thane offer spirometry free of charge, but the waiting lists stretch for weeks. At KEM Hospital in Parel, the pulmonary function test lab sees roughly 40 patients per day, with a backlog that means non-urgent referrals wait a month or more. For a worker who lives in Bhiwandi and must travel two hours each way by train, a single appointment consumes a full day of wages. Many workers told researchers that they simply cannot afford the time. They wait until breathlessness becomes severe enough that they cannot climb a flight of stairs—by which point the disease has often progressed to stage 3 or 4.
The financial barrier is compounded by a lack of awareness. In a 2023 study published in the Indian Journal of Occupational Health, nearly 60% of textile workers surveyed in Mumbai's informal sector had never heard of spirometry. They described their symptoms as “normal” for someone who works with cotton. One worker in the study said, “Everyone in my unit coughs. It means you are working hard.” That normalization of symptoms, combined with the cost of testing, means that many workers are diagnosed only when they land in the emergency room with an acute exacerbation.
Private clinics in the area sometimes offer spirometry at a discount during health camps, but these are sporadic. A SEWA-affiliated health camp in Bhiwandi in late 2024 offered spirometry for ₹200, attracting over 300 workers in one day. But such camps reach a fraction of the estimated 200,000 powerloom workers in the region. For the rest, the test remains a one-time expense that feels out of reach.
Cotton Dust and Fumes: The Everyday Exposure That Silently Destroys Lungs
The cotton that passes through a powerloom shed is not clean. Raw cotton contains dust, bacteria, fungi, and endotoxins released from the plant cell walls. When workers inhale these particles day after day, the lungs mount an inflammatory response. Over years, that inflammation can lead to byssinosis—a disease known colloquially as “Monday fever” because symptoms are worst on the first day back after a break—as well as chronic bronchitis and chronic obstructive pulmonary disease (COPD).
An Indian Council of Medical Research (ICMR) study from 2024, published in the Journal of Occupational and Environmental Medicine, examined 1,200 textile workers across 40 powerloom units in Maharashtra. It found that 34% of workers had obstructive lung disease on spirometry, and the prevalence was highest among those who had worked more than ten years in the industry. The study noted that most units had no exhaust fans, no dust extraction systems, and no provision of N95 masks. Workers wore thin cotton cloths over their mouths, which offer little protection against fine particulates.
The small powerloom units that dominate the industry are especially hazardous. Unlike the large composite mills of Mumbai's past, which had some ventilation and safety protocols, today's typical unit is a rented room in a residential building, with 10 to 20 looms packed tightly. The air is thick with lint and the smell of machine oil. Workers stand or sit within arm's reach of the looms, inhaling dust that settles on their clothes, hair, and skin. By the end of an eight-hour shift, a worker's sputum is often grey or brown.
Women, who make up about 40% of the workforce in these units, face additional exposure because they often perform the tasks that generate the most dust: winding, warping, and cleaning the machines. A 2022 study from the National Institute of Occupational Health found that female winders had a 40% higher prevalence of respiratory symptoms than male weavers, partly because they work in enclosed corners where dust accumulates. Pregnant workers continue to work through the third trimester, exposing the fetus to the same endotoxins. The long-term effects on child respiratory health are not well studied, but some researchers suspect a link.
Diagnosis Delayed Until Disease Is Advanced and Irreversible
When workers finally seek medical help, they often end up at a primary health centre (PHC) where spirometry is not available. A PHC in Bhiwandi sees roughly 200 patients per day, and the doctor on duty has, on average, seven minutes per consultation. In that time, a cough and shortness of breath are likely to be treated with a course of antibiotics and a cough syrup, not a referral for lung function testing. One PHC medical officer told researchers that she rarely orders spirometry because “the machine is broken” or “there is no trained technician.”
Dr. Meena Shah, a pulmonologist at KEM Hospital who has treated textile workers for two decades, estimates that roughly 70% of her patients from the powerloom sector present at stage 3 or 4 COPD, when the lung function is below 50% of predicted. “They come in with oxygen saturation in the 80s, using accessory muscles to breathe,” she said in an interview for this story. “When I ask why they waited, they say they thought it was just a cough. They did not know that shortness of breath is not normal.” By that stage, the damage is largely irreversible in most cases. Treatment focuses on managing symptoms and slowing progression, but the lost lung function does not return.
The delay is not only about cost. Many workers fear that a diagnosis of occupational lung disease will cost them their job. In the informal powerloom sector, there are no formal contracts, no sick leave, and no disability compensation. Employers can dismiss a worker who is perceived as weak or a liability. A 2021 study by the Tata Institute of Social Sciences found that 45% of textile workers who reported respiratory symptoms to their supervisor were assigned lighter work or laid off within three months. The fear is rational: a diagnosis can mean destitution.
Even when a worker reaches a specialist, the diagnostic process can be incomplete. Spirometry requires the patient to take a deep breath and exhale forcefully into a mouthpiece. For a worker with advanced disease, that maneuver is exhausting and may not yield reliable results. Some clinicians rely on peak flow meters or symptom questionnaires instead, but these are less accurate. The gold standard—full pulmonary function testing with bronchodilator response—is available only at tertiary hospitals and costs ₹1,500 or more. Most workers never get it.
Inhalers, Physiotherapy, and the Cost of Living with COPD
Once diagnosed, a textile worker with COPD faces a monthly medication bill that can eat up a third of their income. A basic combination inhaler—a long-acting beta-agonist plus a corticosteroid—costs between ₹800 and ₹1,200 per month at retail prices in Mumbai. For a worker earning ₹10,000 per month, that represents 8–12% of household income. Many workers stretch the inhaler by using it only when symptoms are severe, which leads to more frequent exacerbations and faster decline.
Cheaper alternatives exist, such as oral theophylline tablets that cost about ₹200 per month, but these are less effective and have more side effects, including nausea and heart palpitations. Some workers switch between medications based on what they can afford in a given month. Dr. Shah says she has seen patients who stop taking their inhaler altogether during the rainy season when work is scarce. “They come back in June with an exacerbation that could have been prevented,” she said. “The cost of a hospital admission is far higher, but that is a future expense they cannot think about when they have to feed their children today.”
Pulmonary rehabilitation—a structured programme of exercise, breathing techniques, and education—is nearly nonexistent in the public system for these workers. KEM Hospital runs a rehab programme for COPD patients, but it has capacity for 20 people per session, and the waiting list is six months long. The programme requires patients to attend twice a week for eight weeks, which is impossible for a worker who cannot afford to lose a day's wages. As a result, most workers rely on simple advice: walk a little every day, avoid smoke, use a fan to cool the face. The disease progresses.
The financial toll extends beyond medications. Frequent exacerbations—periods when symptoms worsen suddenly—force workers to take unpaid leave. A single exacerbation that requires a hospital stay of three to five days can cost ₹10,000–15,000 in a public hospital and more in a private one. Families borrow from moneylenders at interest rates of 2–5% per month, falling into a cycle of debt. A 2023 study in the Economic and Political Weekly tracked 100 textile-worker households in Bhiwandi and found that 70% had taken loans for healthcare in the previous year, and the average debt was ₹18,000—nearly two months' income.
Why the System Fails to Catch Occupational Lung Disease Early
India's Factories Act, 1948, requires employers to maintain a “healthy working environment” and to provide medical examinations for workers exposed to hazardous processes. But enforcement is weak. The factory inspectorate in Maharashtra has roughly 200 inspectors for an estimated 50,000 registered factories, and the powerloom units—many of which are unregistered—are rarely inspected. A 2022 report by the Comptroller and Auditor General found that 60% of textile units in Maharashtra had not been inspected in the previous three years. Penalties for violations are low, typically a few thousand rupees, and do not deter employers.
There is no mandatory spirometry screening for textile workers in India, unlike the chest X-ray requirements for silica-exposed workers in some states. The Directorate General of Factory Advice and Service and Labour Institutes (DGFASLI) has published guidelines for occupational health surveillance in the textile industry, but they are advisory, not binding. Most employers do not offer any health check-ups. A 2024 survey by the Centre for Labour Research and Action found that only 8% of powerloom workers in Bhiwandi had ever had a lung function test, and none had been tested at the employer's expense.
Trade unions in the textile sector have long demanded regular health screenings, but their bargaining power is limited. The workforce is fragmented across thousands of small units, and union membership is low—estimated at less than 5% of powerloom workers. The few unions that exist, such as the Bhiwandi Powerloom Workers' Union, focus on wage disputes and safety issues like machine guards, not respiratory health. When workers report symptoms, they risk being labeled as troublemakers. “If you complain about dust, the owner says you are not fit for the job,” said a union organizer who asked not to be named. “So people stay quiet.”
The government's response has been piecemeal. The National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD) includes COPD as a target condition, but its screening efforts are focused on the general population aged 30 and above, not on occupational groups. A pilot project in 2023 to train PHC doctors in spirometry for occupational lung disease was launched in three districts of Gujarat but has not been expanded to Maharashtra. The result is that a preventable disease continues to be diagnosed late, at high cost to individuals and to the health system.
Community Health Workers Offer a Low-Cost Way to Screen Lungs
Despite these gaps, SEWA has trained a cadre of peer educators in Bhiwandi to conduct basic respiratory health assessments using handheld spirometers. The devices, which cost about ₹15,000 each, are simple to use: the worker takes a deep breath and blows into a disposable mouthpiece, and the device calculates the forced expiratory volume in one second (FEV1) and the ratio to forced vital capacity (FVC). The test takes five minutes and costs roughly ₹200 per person when amortized over many uses.
A pilot programme run by SEWA in 2024 screened 800 workers in 20 powerloom units. The peer educators, all women who had worked in the industry themselves, explained the purpose of the test in Marathi and Hindi and addressed fears about job loss. Of those screened, 60% had an abnormal result—an FEV1 below 80% of predicted—and were referred to the public hospital in Thane for confirmatory testing. About half of those referred actually went, and of those, 75% were diagnosed with COPD or byssinosis. The programme cost about ₹160 per person screened, including training and transport.
The model is promising but faces barriers to scale. The handheld spirometers need calibration every six months, and the mouthpieces are single-use, adding to the per-test cost. The peer educators are volunteers who receive a small honorarium of ₹500 per camp day, but they cannot afford to miss their own work. SEWA has applied for funding from the state health department to expand the programme to 5,000 workers, but as of mid-2025, the proposal was still under review. “We have shown that it works,” said a SEWA coordinator. “Now we need the government to see it as a priority.”
Other low-cost innovations include smartphone-based spirometry apps that use the phone's microphone to estimate lung function. A 2023 study from the University of California, San Francisco, tested an app called SpiroSmart in a cohort of textile workers in Bangladesh and found that it detected moderate-to-severe COPD with 85% accuracy compared to standard spirometry. The app is free and requires no hardware beyond a smartphone, which many workers already own. But it has not been validated in Indian populations, and the accuracy for mild disease is lower. Researchers at the Public Health Foundation of India are planning a validation study in Bhiwandi, but funding is uncertain.
Case Study: How Early Screening Changed One Worker's Course
Among the 800 workers screened in the SEWA pilot was 42-year-old Asha Patil, a winder in a Bhiwandi unit for 18 years. She had been coughing for years and assumed it was part of the job. At the SEWA camp, her FEV1 was 65% of predicted—moderate obstruction. She was referred to Thane Civil Hospital, where a confirmatory spirometry confirmed moderate COPD. She was started on a low-dose inhaler and given education on avoiding triggers. “I used to think I would die coughing,” she said in an interview. “Now I use the inhaler every morning, and I can walk to the market without stopping.” Asha still works, but she now wears an N95 mask provided by SEWA and takes short breaks when she feels breathless. She has not had an exacerbation requiring hospitalization in the 18 months since her diagnosis. Her story illustrates that early detection, when combined with affordable treatment and simple protective measures, can alter the trajectory of the disease—even if the underlying lung damage cannot be reversed.
The question is whether these community-based models can be sustained without government backing. SEWA's pilot reached 800 workers out of an estimated 200,000 in the region. To cover even a fraction of that population would require a network of trained screeners, a reliable supply chain for devices and consumables, and a referral system that ensures workers actually receive follow-up care. None of that exists at scale today. The pilot shows what is possible; it does not yet show what is probable.
The story of Shabana Sheikh is not unique. She has not had a spirometry test, but she knows her lungs are not what they were. She has heard about the SEWA camp from a neighbour and plans to attend the next one, if it happens. “If they tell me I have a disease, what will I do?” she asks. “I cannot stop working. My children need to eat.” For now, she keeps a cloth over her mouth and a cough syrup in her bag. She hopes that is enough.
Community screening offers a path forward, but it cannot succeed in isolation. Without employer accountability, government investment, and a safety net for workers who lose income when they seek care, even the most efficient screening programme will reach only a fraction of those in need. The powerloom workers of Bhiwandi and beyond need not just a test they can afford, but a system that values their lungs while they are still working.
This article is for informational purposes only and does not constitute medical advice. Individuals with respiratory symptoms should consult a qualified healthcare provider.