Rajasthan Public Hospitals Offer Free Radiotherapy While Linear Accelerator Downtime Reaches Six Months
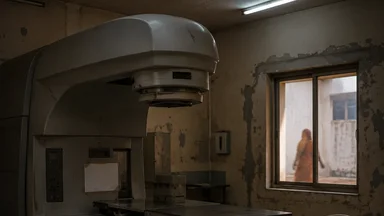
In 2022, Rajasthan announced a policy that seemed like a lifeline for cancer patients: free radiotherapy at all public hospitals across the state. For the roughly 40,000 new cancer cases diagnosed annually in Rajasthan, the promise meant that cost would no longer be a barrier to a critical treatment modality. But nearly two years later, the policy has hit a wall. Linear accelerators—the sophisticated machines that deliver precisely targeted radiation—are breaking down with alarming frequency, and when they fail, they stay broken for months. The gap between policy intent and operational reality is measured in the idling of multi-million-rupee machines while patients wait, their tumours growing.
Free Radiotherapy, But Machines Sit Idle
Rajasthan's free radiotherapy scheme, launched under the state's universal health coverage initiative, covers all government-run medical colleges and district hospitals. The policy eliminates out-of-pocket payments for radiation sessions, a significant relief for families who often spend thousands of rupees on private treatment. However, the programme did not anticipate the frequency and duration of equipment breakdowns. As of late 2024, roughly one-third of the state's linear accelerators were non-functional, according to state health department records cited by local media. The average downtime for a broken machine was about six months, with some machines idle for over a year.
When a linear accelerator fails, patients are placed on waiting lists for nearby working machines. Those who cannot wait are referred to private centres, where a course of radiotherapy can cost between 50,000 and 150,000 rupees—a sum that for many families is catastrophic. The state's free treatment policy does not cover these private referrals, so patients face a cruel choice: wait for an uncertain repair date or pay for treatment they cannot afford. The policy thus creates a two-tier system: those with means bypass the queue, while the poor wait—and sometimes wait too long.
The root of the problem lies not in the purchase of equipment but in its maintenance. Rajasthan's health budget allocates funds for capital expenditure on new machines but provides little for ongoing servicing. Annual maintenance contracts with manufacturers, which cost roughly 10–15% of the machine's value, have lapsed in at least six districts, including Bhilwara, Dungarpur, Sirohi, Churu, Hanumangarh, and Banswara, according to a 2024 report by the Rajasthan State Health Systems Resource Centre. In Bhilwara, the contract expired in early 2023 and was not renewed for 14 months; in Dungarpur, no contract was ever signed after installation. The state's procurement system treats the linear accelerator as a one-time purchase, ignoring that these machines require skilled engineers, spare parts, and regular calibration to function safely and effectively.
This policy gap is not unique to Rajasthan. Across India, public hospitals struggle with equipment maintenance. A 2023 study in the Indian Journal of Medical Ethics found that nearly 40% of medical equipment in district hospitals was non-functional at any given time. In Rajasthan, that figure for radiotherapy-specific equipment was even higher: the same study reported that 48% of linear accelerators in the state's district hospitals were non-functional at the time of the survey, compared to a national average of 34%. The consequences are especially acute for radiotherapy, where delays directly affect survival. For cervical cancer—one of the most common cancers among women in Rajasthan—radiotherapy is often the primary treatment, and a delay of even a few weeks can reduce the chance of cure.
Why Linear Accelerators Break and Stay Broken
Linear accelerators are among the most complex machines in a hospital. They generate high-energy X-rays or electrons by accelerating electrons through a waveguide and colliding them with a target. The technology requires precise calibration, temperature control, and regular maintenance. A single breakdown can involve anything from a faulty magnetron to a software glitch. Repairing these machines demands specialised biomedical engineers—a rare skill in Rajasthan, where most technicians are trained in general electronics, not radiotherapy-specific systems.
The state has only a handful of engineers capable of servicing linear accelerators, and they are concentrated in the larger cities like Jaipur and Jodhpur. When a machine fails in a district hospital, a technician must travel from the city, often days or weeks later. Even then, the problem may require a spare part that is not in stock. Many parts are imported—from the United States, Germany, or Japan—and customs clearance can take weeks. A 2024 audit by the Rajasthan State Health Systems Resource Centre found that spare part delays accounted for roughly 40% of total downtime.
There is no central repair pool across Rajasthan's cancer hospitals. Each facility manages its own maintenance, leading to duplication of effort and inconsistent expertise. For example, the Sawai Man Singh (SMS) Medical College in Jaipur attempted to train two local engineers through a six-month course at the Christian Medical College in Vellore, but both left for private-sector jobs within a year. In Bhilwara, the hospital sent a technician for a two-week workshop at the manufacturer's facility in Mumbai, but the training was too short to cover complex repairs. Without a systemic approach, the cycle of breakdown and delayed repair continues. The state's reliance on manufacturer service contracts, which are expensive and often slow, exacerbates the problem. A more coordinated model—such as a state-level maintenance unit—could pool resources and expertise, but such an initiative has not been prioritised.
The Burden Falls on Cervical Cancer Patients
Cervical cancer is the second most common cancer among women in Rajasthan, with an incidence rate of roughly 22 per 100,000, according to the National Cancer Registry Programme. Each year, an estimated 6,000 women in the state are diagnosed with cervical cancer, and about half of them present with advanced-stage disease, for which radiotherapy is the mainstay of treatment. The standard regimen involves daily sessions for five to six weeks, often combined with chemotherapy. Any interruption or delay can compromise outcomes.
A landmark study published in The Lancet in 2023 found that a delay of more than six weeks between diagnosis and the start of radiotherapy was associated with a 10–15% increase in mortality for cervical cancer patients. The study, which pooled data from over 10,000 women across low- and middle-income countries, underscored the importance of timely treatment. In Rajasthan, where machine downtime can stretch to six months, many patients face delays far exceeding that threshold. The result is preventable deaths.
Rajasthan has made strides in cervical cancer screening, with free Pap smears and HPV testing at primary health centres under the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke. But screening is only half the battle. When a woman is diagnosed with cervical cancer, she needs access to treatment—and that treatment chain is only as strong as its weakest link. The state's investment in early detection is undermined by the failure to ensure that radiotherapy machines are operational. As Kerala Pap Smear Rates Stay Low While HPV Self-Sampling Trials Show Promise, Rajasthan's screening rates are also suboptimal, but even women who are diagnosed face a broken system.
For women in rural areas, the burden is compounded by travel costs. A patient from a village in Barmer district, where no linear accelerator exists, must travel to Jodhpur—a distance of roughly 200 kilometres—for treatment. If the Jodhpur machine is also broken, she may be referred to Jaipur, another 300 kilometres. The cost of transport, accommodation, and lost wages can be as high as the treatment itself. Many women abandon treatment altogether. A 2024 study from the Indian Institute of Health Management Research in Jaipur found that 30% of cervical cancer patients in Rajasthan did not complete their prescribed radiotherapy course, with machine breakdown cited as the primary reason.
A Tale of Two Hospitals: Jaipur vs. Bhilwara
Sawai Man Singh (SMS) Medical College in Jaipur is the state's flagship cancer centre, with three linear accelerators. As of late 2024, two were operational. The third had been down for four months due to a faulty modulator, a key component that controls the electron beam. The hospital's biomedical engineering team attempted repairs but lacked the specialised knowledge to fix it. A technician from the manufacturer was called, but his visit was delayed by two months due to scheduling conflicts. During that time, patients were diverted to the two working machines, which operated at near full capacity. Wait times for a new patient to start radiotherapy stretched from two weeks to six weeks.
In Bhilwara district hospital, the situation is far worse. The hospital received its first linear accelerator in 2021 as part of a central government scheme to upgrade district hospitals. The machine, a refurbished model from a European manufacturer, worked for just over a year before developing a recurring fault in the gantry rotation system. The annual maintenance contract had been signed for only one year and was not renewed. By early 2023, the machine was non-functional. As of mid-2024, it had been idle for eight months. The hospital refers all radiotherapy patients to SMS Medical College in Jaipur, 150 kilometres away. For many, the journey is prohibitively expensive.
The disparity between Jaipur and Bhilwara illustrates a broader inequity in Rajasthan's cancer care. Urban centres with medical colleges have multiple machines and some engineering capacity, while district hospitals are left with a single machine and no backup. When that machine fails, the entire district's radiotherapy needs go unmet. The state's policy of free treatment applies uniformly, but access to treatment is anything but uniform. Patients in districts like Bhilwara, Dungarpur, or Sirohi effectively have no access to free radiotherapy, despite the policy's promise.
This geographic inequity is not unique to Rajasthan, but it is particularly stark because of the state's size and low population density. A patient in a remote district may need to travel 200–300 kilometres for treatment, which is not feasible for many. The state government has proposed setting up tele-radiotherapy consultation centres, but these cannot replace a functioning machine. The only real solution is to ensure that every district hospital's linear accelerator works reliably, which requires a maintenance system that currently does not exist.
Policy Fixes That Could Halve Downtime
Reducing linear accelerator downtime in Rajasthan is not technically impossible, but it requires a shift in how the state thinks about equipment maintenance. The first step is to establish a state-level maintenance contract with a single private vendor, covering all public hospitals. Such a contract would guarantee response times, spare parts availability, and regular preventive maintenance. A similar model has been used in Tamil Nadu for CT scanners, with measurable reductions in downtime. Rajasthan's health department could adapt this approach, using a performance-based contract that penalises the vendor for delays.
Second, the state should invest in training biomedical engineers specifically in radiotherapy technology. India has several institutes, such as the Indian Institute of Technology and the Christian Medical College in Vellore, that offer specialised courses in medical equipment maintenance. Rajasthan could sponsor a cohort of engineers to undergo such training, with a commitment to serve in public hospitals for a minimum period. This would create a pool of local expertise, reducing dependence on manufacturer technicians who are often based in other states.
Third, a central spare-part stockpile should be created, similar to the vaccine cold chain system that India uses for immunisation programmes. The stockpile would hold commonly needed parts—magnetrons, waveguides, cooling pumps—at a central warehouse in Jaipur, with a logistics system to dispatch them within 48 hours. This would eliminate customs delays for individual hospitals and reduce downtime. The initial investment would be roughly 10–20 million rupees, but the savings from reduced patient referrals and improved outcomes would far outweigh the cost.
Finally, tele-mentoring for troubleshooting, as pioneered by the All India Institute of Medical Sciences (AIIMS) in New Delhi, could help district-level technicians diagnose and fix simpler problems without waiting for a visit. AIIMS runs a remote support programme for ultrasound machines in rural clinics, where a technician in a village can share a video feed of the machine's error code with an expert in Delhi. A similar system for linear accelerators could resolve perhaps 20–30% of breakdowns within hours, rather than weeks. These four interventions together could realistically halve the average downtime from six months to three months—a significant improvement, though still far from ideal.
Trade-Offs and Challenges
While these policy fixes are promising, they come with trade-offs that require careful consideration. Establishing a state-level maintenance contract, for instance, may reduce flexibility for individual hospitals and could lead to vendor lock-in. If the chosen vendor underperforms or goes out of business, the entire state's radiotherapy services could be affected. Diversifying vendors across districts might mitigate this risk but would increase administrative complexity.
Training biomedical engineers is a long-term investment that may not yield immediate results. The state would need to offer competitive salaries and career progression to retain trained engineers, as the private sector often poaches skilled personnel. A bond system requiring engineers to serve in public hospitals for a minimum of five years could help, but enforcement is difficult. Moreover, the initial cost of training a cohort of 10–15 engineers could be 5–10 million rupees, which must be weighed against other pressing health needs.
Creating a central spare-part stockpile requires upfront capital and ongoing logistics management. The stockpile must be regularly audited to prevent expiry or obsolescence of parts, and the warehouse needs climate control to preserve sensitive components. The state would also need to negotiate with multiple manufacturers to ensure compatibility of parts across different machine models. Failure to do so could result in a stockpile of unusable parts.
Tele-mentoring for troubleshooting assumes that district-level technicians have basic diagnostic skills and reliable internet access, which is not always the case in remote Rajasthan. Power outages and connectivity issues could render the system ineffective for a significant proportion of breakdowns. A hybrid approach—where tele-mentoring is supplemented by periodic on-site visits from a central team—may be more realistic but would increase costs.
There is also the fundamental question of resource allocation. Every rupee spent on maintaining old machines is a rupee not spent on purchasing new ones. Newer linear accelerators are more reliable and require less frequent maintenance, but they cost 50–70 million rupees each. Rajasthan must decide whether to invest in a maintenance overhaul for its existing fleet or to gradually replace machines with newer models. A cost-benefit analysis by the state's health department in 2023 suggested that a mixed strategy—maintaining functional machines while phasing out the oldest ones over five years—would be most cost-effective, but this has not been implemented.
Finally, the political economy of health budgets cannot be ignored. Maintenance funds are often the first to be cut during fiscal tightening, as they lack the visibility of new construction or equipment purchases. Advocacy groups like the Rajasthan Cancer Society have called for a dedicated maintenance fund ring-fenced from the general health budget, but this requires legislative action. Without such protection, even the best-laid plans may falter when budgets are squeezed.
What Other States Can Learn from Rajasthan
Rajasthan's struggles are not unique, but they offer lessons for other states that are expanding cancer care infrastructure. Tamil Nadu, for instance, has implemented a hub-and-spoke model for equipment repair, where a central workshop in Chennai services machines from district hospitals across the state. The workshop employs engineers trained by manufacturers and maintains a stock of spare parts. As a result, the average downtime for CT scanners in Tamil Nadu's public hospitals is under two weeks, compared to months in many other states. Kerala, too, has invested in in-house engineering teams at its major cancer centres, with dedicated technicians who perform preventive maintenance and minor repairs on site. The Kerala Pap Smear Rates Stay Low While HPV Self-Sampling Trials Show Promise illustrates that even with better maintenance, screening and treatment must go hand in hand.
The National Cancer Grid, a network of cancer centres across India, has developed procurement guidelines that include mandatory maintenance contracts for at least five years after installation. These guidelines are not binding, but states that follow them—such as Karnataka and Gujarat—report lower downtime. The central government's Ayushman Bharat scheme could also tie funding for new equipment to a maintenance plan, ensuring that states budget for repairs from the outset. Without such conditions, the cycle of purchase, breakdown, and neglect will repeat.
Budget allocation is the crux. A linear accelerator costs roughly 50–70 million rupees, but its 10-year maintenance costs add another 70–100 million rupees. Many states, including Rajasthan, allocate only the purchase price. The result is a fleet of machines that age prematurely and fail frequently. International experience, such as the World Health Organization's guidelines on medical equipment maintenance, recommends that 5–10% of the initial purchase cost be set aside annually for maintenance. For Rajasthan's roughly 15 linear accelerators, that would mean an additional 50–100 million rupees per year—a small fraction of the state's health budget, but a recurring expense that must be planned for.
The lesson is clear: a cancer treatment policy is only as good as the machines that deliver it. Rajasthan's free radiotherapy scheme is a noble goal, but without a maintenance strategy, it is a promise that cannot be kept. Other states, especially those with large rural populations, should take note before expanding their own radiotherapy services.
The Cost of Inaction: Preventable Deaths Mount
The human cost of idle linear accelerators is measured in deaths that could have been prevented. Rajasthan records roughly 6,000 cervical cancer cases annually, and about 2,000 women die from the disease each year, according to the Indian Council of Medical Research. If radiotherapy delays contribute a 10–15% excess mortality—conservative, based on the Lancet study—that translates to 200–300 preventable deaths each year from cervical cancer alone. When other cancers that require radiotherapy are included—head and neck, breast, rectal—the number could be far higher.
These deaths are not abstract statistics. They are women like Meena, a 45-year-old mother of three from a village in Bhilwara district, who was diagnosed with late-stage cervical cancer in early 2023. She was referred to Jaipur for radiotherapy, but the wait for a working machine was two months. By the time she started treatment, her tumour had progressed. She died in early 2024. Her family spent over 100,000 rupees on travel and lodging during her treatment, wiping out their savings. Her story is not uncommon. A free treatment policy that cannot be accessed is an ethical failure, and the state bears responsibility.
Rajasthan's next state budget, due in early 2025, must earmark funds specifically for equipment maintenance. The health department has proposed a "repair and maintenance fund" of 200 million rupees, but it has not yet been approved. Advocacy groups, including the Rajasthan Cancer Society, are pushing for this allocation, arguing that it would save more lives than buying new machines. The trade-off is real: every rupee spent on maintenance is a rupee not spent on new equipment, but a functional old machine is better than a broken new one.
The broader lesson is that universal health coverage requires not just financial protection but also functional infrastructure. Rajasthan's free radiotherapy policy is a step in the right direction, but it must be accompanied by a robust maintenance system. Without it, the policy is a promise that cannot be kept, and the most vulnerable patients—those with cervical cancer in rural areas—pay the price.
This article is for informational purposes only and does not constitute medical advice. Individuals with health concerns should consult a qualified healthcare professional.