Dar es Salaam Clinic Offers Free Asthma Inhalers While Spirometry Machines Gather Dust
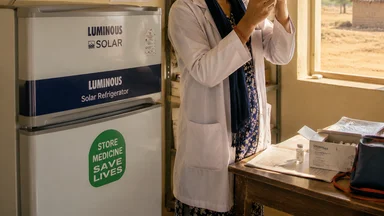
On a dusty side street in Dar es Salaam's Kariakoo district, a public clinic distributes free asthma inhalers to hundreds of patients each month. The inhalers, donated by an international non-profit, arrive in sealed cartons labeled with expiration dates two years out. But in a locked storeroom down the hall, two spirometry machines—donated around the same time—sit in their original packaging, gathering a fine layer of coastal dust. No one at the clinic has been trained to use them, and the service contract that was supposed to include calibration and filter replacement never materialized. This scene, repeated across Tanzania and much of sub-Saharan Africa, captures a paradox at the heart of global respiratory care: treatments flow, but diagnostics stagnate.
The result is a system where patients may receive inhalers for years without ever having their condition confirmed—or they may be treated for asthma when they actually have COPD, tuberculosis, or even heart failure. The disconnect is not merely logistical; it reflects deeper disagreements among experts about what counts as good care in settings where resources are scarce.
Free Inhalers in Dar, Broken Spirometers in Storage
The clinic in Kariakoo is not unique. Across Tanzania, donor-funded asthma medications have become more available in recent years, thanks in part to initiatives like the Global Asthma Network and bilateral health programs. But the diagnostic equipment that should guide their use—spirometers, peak flow meters, and even basic peak flow charts—often lags behind. A 2023 survey of 45 primary care facilities in Dar es Salaam found that 38 had at least one spirometer on site, but only 12 had ever used it, and just 5 had performed a test in the preceding month.
Dr. Amina Mwinyi, a respiratory physician at Muhimbili National Hospital, explains the consequences. “We see patients who have been on inhaled corticosteroids for five years, but when we finally do spirometry, we find they have normal lung function. They may have had a viral wheeze, or even anxiety hyperventilation, not asthma. Meanwhile, a patient with undiagnosed COPD has been getting asthma inhalers that don't help, and their disease progresses.” She estimates that roughly 30 to 50 percent of patients referred to her clinic with a prior diagnosis of asthma turn out to have a different condition after spirometry. A study in Tanzania, published in the International Journal of Tuberculosis and Lung Disease in 2022, found that symptom-based algorithms misclassified about 35 percent of patients with chronic cough, compared with spirometry. The misclassification rate was highest in older adults, where asthma and COPD overlap, and in people with a history of tuberculosis, which can cause permanent lung damage that mimics asthma.
The machines themselves are not inherently fragile. Modern spirometers are robust devices, but they require regular calibration, disposable filters, and a trained operator who can coach patients through forced expiratory maneuvers. In dusty, humid environments with intermittent power, electronic sensors drift. Without service contracts—often omitted from donation agreements—machines break and stay broken. “Donors love to ship boxes of inhalers,” says Dr. Mwinyi. “They can count them, photograph them, report them to headquarters. A spirometer is invisible. It doesn't make a good photo.”
Clinicians at the clinic rely on symptom-based diagnosis: wheezing, shortness of breath, cough, and response to a trial of bronchodilators. This approach, endorsed by some World Health Organization guidelines for primary care in low-resource settings, is pragmatic but imprecise. The cost of misdiagnosis is not just clinical. Inhalers are expensive relative to other essential medicines; a typical course of inhaled corticosteroids costs a donor program around US$10 to $20 per patient per month. When a third of those patients do not have asthma, the waste is substantial. “We are spending money on the wrong patients, and the right patients are not getting the right drugs,” says Dr. Mwinyi. “It's a system failure, but it's a fixable one.”
Why Spirometry Matters and Why It Fails in Low-Resource Settings
Spirometry is the gold standard for diagnosing asthma and COPD. It measures how much air a person can exhale in one second (FEV1) and the total volume exhaled (FVC), producing a ratio that distinguishes obstructive from restrictive lung disease. The test is non-invasive, takes about 15 minutes, and can be performed at the bedside. But in practice, it demands more than hardware. The American Thoracic Society recommends that spirometry be performed by trained personnel, using equipment that meets accuracy standards, with quality control checks at least weekly. In many low-resource settings, these conditions are rarely met.
Donated machines often arrive without accessories. A common scenario: a clinic receives a spirometer but no disposable mouthpieces, no calibration syringe, and no power adapter compatible with local voltage. The manufacturer's software may be in English or French, not Swahili, and the manual may be a dense PDF that no one has time to read. “We opened the box and there was a beautiful machine, but we didn't know what to do with it,” says Sister Grace, a nurse at the Kariakoo clinic. “The person who brought it said training would come, but it never did.” That was three years ago.
Even when training is provided, staff turnover can undo progress. Dr. John Mushi, a pulmonologist at Muhimbili National Hospital, recalls training 15 nurses on spirometry in 2022. By 2024, only three were still at the facility; the rest had transferred or left government service. “Each time we train, we start from zero,” he says. “The knowledge doesn't stay in the system.” This churn is compounded by the fact that spirometry is not a high-volume test in most clinics; a nurse may perform it only once a week, making it hard to maintain proficiency.
Power outages are another obstacle. In Dar es Salaam, grid electricity is unreliable, and many clinics lack backup generators or solar panels. Spirometers with internal batteries can run for a few hours, but if they are not recharged, they fail. Dust and humidity degrade sensors and screens. Some clinics have resorted to storing machines in plastic bags, which traps moisture and accelerates corrosion. “The climate is tough on electronics,” says Dr. Mushi. “But we can't just give up. We need to design systems that work here, not import solutions from Europe.”
The alternative—symptom-based care—has vocal defenders. Dr. James Kilonzo, a general practitioner at a rural health center in Morogoro, argues that spirometry is a luxury in settings where a single doctor sees 100 patients a day. “If a patient has wheeze and responds to a bronchodilator, I treat them for asthma. I don't need a machine to tell me that. The machine would take 15 minutes per patient, and I don't have 15 minutes.” He acknowledges the risk of misdiagnosis but says it is acceptable given the constraints. “In an ideal world, everyone gets spirometry. In this world, we do what we can.”
The Global Disconnect: Donor Priorities vs. Local Needs
The imbalance between inhalers and spirometers is not accidental. It reflects the way global health funding is structured: donors prefer vertical programs that deliver measurable outputs—number of inhalers distributed, patients treated—over horizontal investments in diagnostic infrastructure that are harder to quantify. A 2024 analysis by the World Health Organization of respiratory health funding in sub-Saharan Africa found that for every dollar spent on asthma medicines, less than five cents went to diagnostics, including spirometry, peak flow meters, and training.
The World Health Organization's Essential Diagnostics List includes spirometers for the diagnosis of asthma and COPD, but inclusion does not guarantee procurement. National tenders often prioritize medicines because they are easier to manage and have established supply chains. Diagnostics require additional steps: training, maintenance, quality assurance. “Inhalers come in a box, they have a long shelf life, and you can count them,” says Dr. Mary Mbuya, a health economist at the University of Dar es Salaam. “A spirometer is a capital investment. It needs annual calibration, consumables, and a trained person. Donors are not set up for that.”
Tanzania's national asthma guidelines, updated in 2022, recommend spirometry for diagnosis whenever possible. But the guidelines also acknowledge that most primary care facilities lack the equipment and expertise, and they endorse a symptom-based algorithm as an acceptable alternative. This dual standard—recommending what is ideal while accepting what is feasible—creates a perverse incentive. Clinics are not penalized for failing to perform spirometry, and donors have no reason to fund it when they can point to inhaler distribution numbers instead.
The result is a system that treats symptoms but does not confirm disease. Patients with asthma may be overtreated with high-dose inhalers, while those with COPD may be undertreated because their condition is misclassified. People with post-tuberculosis lung disease—a common sequela in high-burden countries—may be diagnosed with asthma and given inhalers that provide minimal benefit. “We are wasting resources and harming patients,” says Dr. Mbuya. “But the waste is invisible because it happens inside the body, not in the supply chain.”
A similar dynamic plays out in other areas of global health. In Lagos, public clinics stock malaria rapid diagnostic tests while microscopy rates stall, as reported in a recent analysis. In South Africa, antiretroviral drugs flow freely while CD4 machine downtime stretches to five months, as documented here. The pattern is consistent: treatment is visible, diagnostics are not. And without diagnostics, treatment becomes guesswork.
What Experts Disagree On: Is Symptom-Based Care Enough?
The question of whether symptom-based care is sufficient for asthma diagnosis in low-resource settings divides the respiratory medicine community. On one side are pragmatists who argue that in settings where spirometry is unavailable, a careful history and trial of treatment are good enough. They point to studies showing that symptom-based algorithms can correctly identify asthma in about 70 to 80 percent of cases, especially in children and young adults with classic symptoms. “We don't need perfection to save lives,” says Dr. Kilonzo. “We need to treat the people who need treatment and not let the perfect be the enemy of the good.”
On the other side are diagnostic purists who insist that spirometry is essential to avoid both over- and under-treatment. They cite evidence that misdiagnosis rates in primary care can exceed 50 percent, particularly in older adults, smokers, and people with prior lung infections. “Asthma is a clinical diagnosis, but it's not a simple one,” says Dr. Mwinyi. “Without objective lung function, you are guessing. And guessing leads to harm.” A 2023 systematic review by Nantanda et al. in the Journal of Global Health of asthma diagnosis in sub-Saharan Africa found that only 12 percent of diagnosed cases had been confirmed by spirometry. The rest were based on symptoms alone.
The World Health Organization's position is nuanced. Its 2021 package of essential noncommunicable disease interventions for primary care includes spirometry as a recommended diagnostic tool for asthma and COPD, but it also provides a symptom-based algorithm for settings where spirometry is not available. This dual-track approach reflects the reality that universal spirometry is a distant goal. But critics argue that the algorithm is too blunt. It does not distinguish well between asthma and COPD, and it performs poorly in people with a history of tuberculosis, which affects roughly 5 to 10 percent of adults in high-burden countries.
Cost-effectiveness analyses have not settled the debate. A modeling study in Kenya estimated that adding spirometry to primary care would cost about US$50 per correct diagnosis, compared with US$10 for symptom-based diagnosis. But the study also found that spirometry reduced misdiagnosis-related costs—wasted inhalers, unnecessary hospitalizations—by about 30 percent. Whether that trade-off is acceptable depends on the budget holder's perspective. A donor focused on short-term outputs may prefer the cheaper option; a health system planner thinking long-term may invest in diagnostics.
The disagreement is not merely academic. It shapes how international guidelines are written, how national programs are designed, and how millions of patients are treated. In the absence of consensus, the default in most low-resource settings is symptom-based care. “We are making a decision by not making a decision,” says Dr. Mbuya. “And that decision is to accept high rates of misdiagnosis as the price of doing business.”
Learning from Pilot Programs That Made Diagnostics Work
Despite the challenges, several pilot programs have demonstrated that spirometry can be deployed effectively in low-resource settings. In Kenya, a pulmonology training program led by the Kenya Association of Pulmonologists and the American Thoracic Society trained 60 nurses and clinical officers in spirometry over two years. Participating clinics saw a fourfold increase in spirometry use, and the proportion of asthma diagnoses confirmed by objective testing rose from 15 percent to 55 percent. The key was not just training, but ongoing mentorship: a pulmonologist visited each clinic quarterly to review technique and provide feedback. The program also provided a simple, rugged device—the EasyOne spirometer—that can withstand dust and humidity, and it ensured a supply of consumables by budgeting for them from the start. “The technology is not the bottleneck,” says Dr. Mwinyi. “The bottleneck is the system around the technology. If you fix the system, the machine works.”
In South Africa, mobile spirometry units have brought diagnostics to rural communities in the Eastern Cape. The units, mounted in vans equipped with solar panels and backup batteries, travel a circuit of clinics, performing tests on site and sending results electronically to a central reading center. A 2024 evaluation published in the South African Medical Journal found that the program reduced the time to diagnosis from an average of six months to two weeks, and that 40 percent of patients referred for spirometry had a diagnosis different from their initial clinical impression. The cost per test was about US$25, comparable to the cost of a month of inhalers. The mobile units also allowed for quality assurance: a specialist in Cape Town reviewed every test result remotely, ensuring that accuracy was maintained even in remote areas.
Tanzania has its own pilot to learn from. In Mwanza, a partnership between the Tanzanian Ministry of Health and the University of Cambridge introduced spirometry at three district hospitals, along with training for local technicians and a telemedicine link to a specialist in Dar es Salaam. Over 18 months, the program performed more than 2,000 tests and reduced the misdiagnosis rate among referred patients from 45 percent to 18 percent. The program was funded by a research grant, but its operational costs were modest: roughly US$15 per test, including consumables and staff time. The success of the Mwanza program has led to discussions about scaling it to other regions, though funding remains uncertain.
What these programs share is a focus on local capacity rather than hardware. They trained existing staff—nurses, clinical officers—rather than relying on scarce specialists. They ensured a supply of consumables by budgeting for them from the start. They used simple, rugged devices that can withstand dust and humidity. And they built in quality assurance through telemedicine or periodic visits. But pilots are not scale. Replicating these successes across hundreds of clinics requires sustained funding, political will, and a shift in donor priorities. “We have the evidence that it works,” says Dr. Mbuya. “What we don't have is the commitment to make it routine.”
Another promising example comes from Uganda, where a pilot program integrated spirometry into existing tuberculosis screening services at primary care clinics. By co-locating spirometry with TB diagnostic services, the program leveraged existing laboratory infrastructure and trained staff. A 2023 evaluation found that the cost per spirometry test dropped by 40 percent when shared with TB services, and that the integrated approach improved detection of both TB and COPD in patients with chronic cough. The program also trained nurses to perform spirometry, which reduced the burden on doctors and increased test availability. “Integration is the way forward,” says Dr. Mbuya. “We don't need separate systems for every disease. We need to build platforms that can handle multiple conditions.”
Policy Fixes: From Vertical Programs to Integrated Lung Health
Moving from pilots to national programs will require policy changes at multiple levels. One promising approach is to integrate spirometry into existing vertical programs, such as those for tuberculosis and HIV. In many clinics, TB and HIV services already have laboratory infrastructure, trained staff, and reliable supply chains. Adding spirometry to these platforms could leverage existing capacity and reduce per-test costs. A pilot in Uganda that co-located spirometry with TB screening found that the cost per test dropped by 40 percent when shared with TB diagnostic services.
Another fix is to train nurses and clinical officers to perform and interpret spirometry, rather than relying on doctors. Task-shifting is common in other areas of global health—HIV testing, cervical cancer screening—and has been shown to be safe and effective for lung function testing. A study in Malawi found that nurses who completed a two-day training could perform spirometry with accuracy equivalent to that of specialists, as long as they had access to periodic quality review.
Donors, too, must change their approach. Rather than donating machines without service contracts, they could bundle spirometers with a multi-year commitment to consumables, training, and maintenance. Some organizations, like the Global Fund, have begun to include diagnostics in their funding proposals for noncommunicable diseases, but the amounts remain small relative to medicines. “We need to convince donors that a spirometer is not a one-time purchase, it's an ongoing investment,” says Dr. Mbuya. “And that investment pays for itself by reducing waste.”
National health insurance schemes, where they exist, could also play a role. In Tanzania, the National Health Insurance Fund covers asthma medications but does not reimburse spirometry. Adding spirometry to the benefits package would create a financial incentive for clinics to offer the test, and for patients to demand it. “Right now, there is no financial reason for a clinic to do spirometry,” says Dr. Mwinyi. “If we make it reimbursable, that changes the calculus.”
Tanzania's new Noncommunicable Disease Strategy, launched in early 2026, includes a goal of increasing spirometry availability at district hospitals to 80 percent by 2030. The strategy also calls for integrating lung health services into primary care and training 500 health workers in spirometry over five years. Whether these goals will be met depends on funding and implementation. “The strategy is good on paper,” says Dr. Mbuya. “The question is whether we can execute it. We have the plan. Now we need the resources and the will.”
The disconnect between treatment and diagnostics in global respiratory care is not inevitable. The examples from Kenya, South Africa, and Uganda show that with the right approach—local training, integrated platforms, sustained investment—spirometry can become a routine part of primary care even in the most resource-constrained settings. The challenge is not technical; it is political and financial. Until donors and governments treat diagnostics as a core component of care, rather than an afterthought, the inhalers will keep flowing, and the spirometers will keep gathering dust.